In 2013, Genesis Fertility Centre became the first and only clinic in Canada to independently verify our clinical results. We did this to improve transparency about our clinic�s pregnancy rates and translate for patients procedural success rates that are often reported in different ways.
In the U.S., reporting of pregnancy rates by fertility clinics is mandatory, audited and identifiable. In Canada, reporting is voluntary, de-identified and unaudited. Websites may contain only biochemical pregnancy rates* and use different denominators, making it virtually impossible for patients to compare the success rates of different fertility clinics.
At Genesis, we ensure validity of our pregnancy rates annually through third-party auditing conducted by two independent, unrelated industry organizations: Fertility Authority, a leading authority in patient advocacy, and IVF Reports, an authority in IVF standards.
At Genesis Fertility Centre, we believe that singleton pregnancies are healthiest for mothers and babies as multiple implantation’s increase the risk of pre-term delivery and obstetrical complications.
Between January 2011 and December 2012, Genesis�s elective and mandatory single embryo transfer rate was 18%.
In 2013, elective day-five single embryo (eSET) utilization increased to 76% for eligible women under age 37 (table 3).
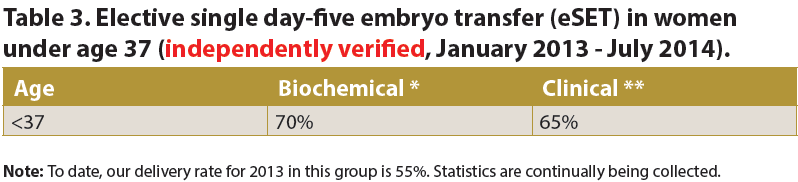
What do these numbers mean?
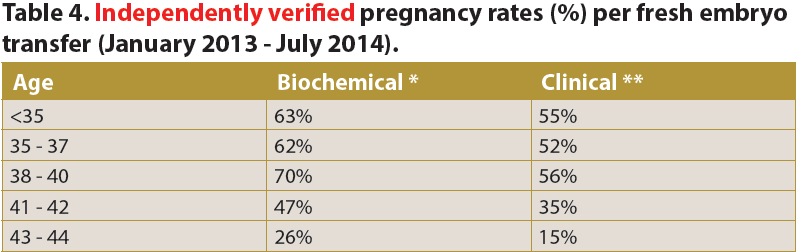
Pregnancy rates may be reported in several ways due to various definitions of�pregnancy (see Table 4). The denominator against which positive pregnancies are measured also vary:
- The start of an IVF cycle, i.e. the start�of fertility medication
- Egg retrieval
- Embryo transfer
We report according to fresh embryo transfer.
Why do we report according to fresh embryo transfer?
Many patients now choose to freeze their embryos for later use rather than proceed with embryo transfer immediately. Also, some patients with poorer prognoses or more challenging histories (e.g. AMH levels of <0.5; multiple previous failed cycles at the same or different fertility�clinics) may have poorer progression to transfer, i.e. no embryo to transfer. In the past, these patients may have been denied a chance to try. We take pride in accepting these �challenging cases� provided the patients understand the prognoses.�We are honoured to help them build their�families.
Not all egg retrievals result in embryo transfer:
- Fertility preservation for patients�with cancer or other medical issues
- �Cryopreservation of embryos for�later use due to:
i. Genetic screening (day-five�embryo biopsy and freezing while�awaiting results of testing)
ii. Risk of ovarian hyperstimulation
iii. Uterine factor infertility
iv. Other, e.g. personal or health�reasons
- No eggs retrieved (this occurs at a�frequency of <1% in a normal�responder)
- �Failed fertilization (occurs in <5% of�cases)
- Failed embryo development (occursin <1% of cases)
We intend to post our pregnancy rates�according to age, AMH levels and previous�attempts on our website to allow patients�to interpret their individual circumstances.�Stay tuned!
*Biochemical pregnancy rates are defined as positive blood tests done 17 days after the embryo transfer.